25 year old gentleman with bike on car collision admitted with left hypochondrial pain and severe tenderness. The chest x-ray did not show any rib fracture. The blood pressure was stable. Urine showed microscopic haematuria.
Image gallary:
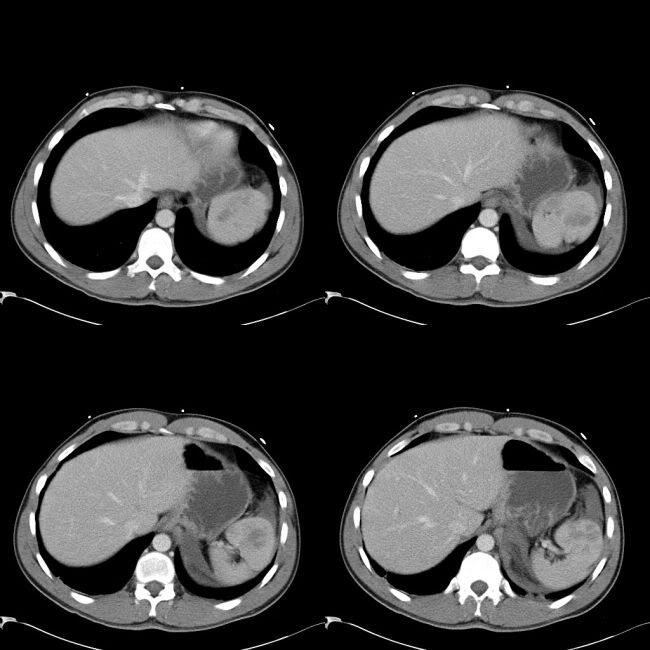
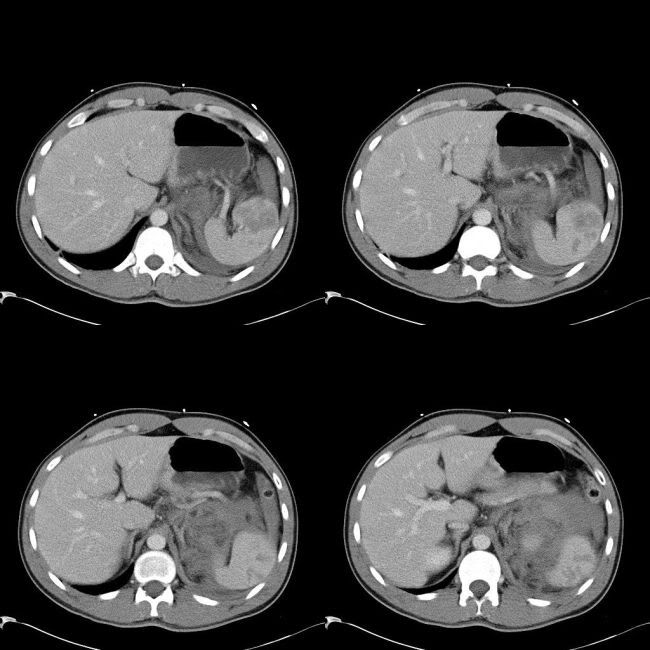
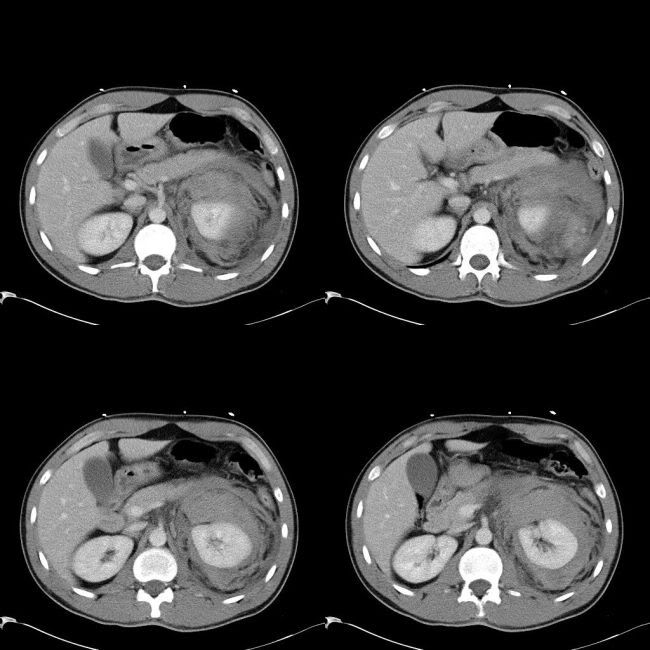
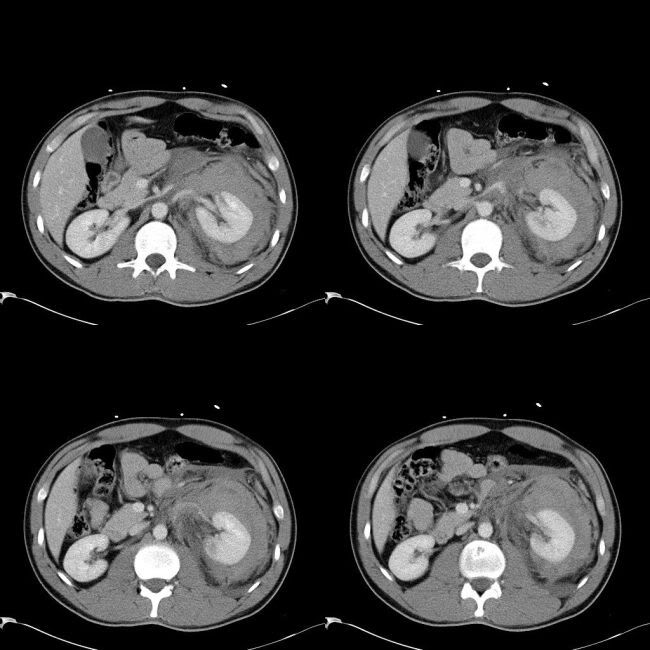
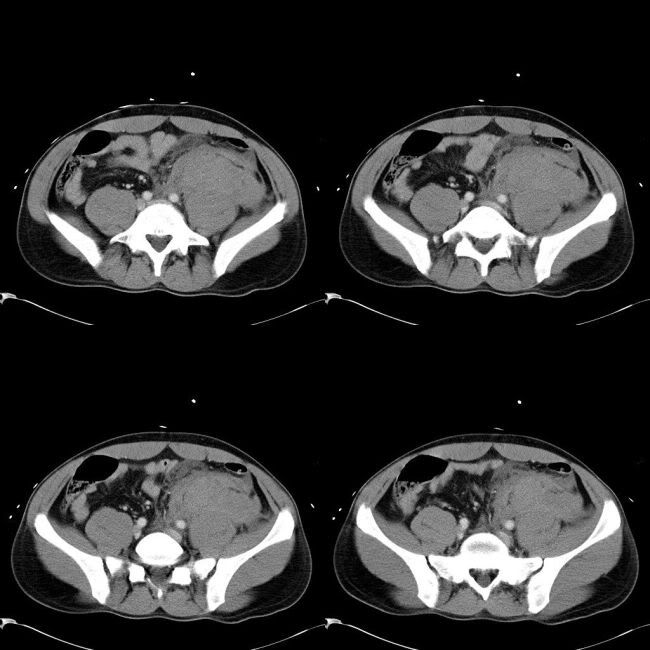
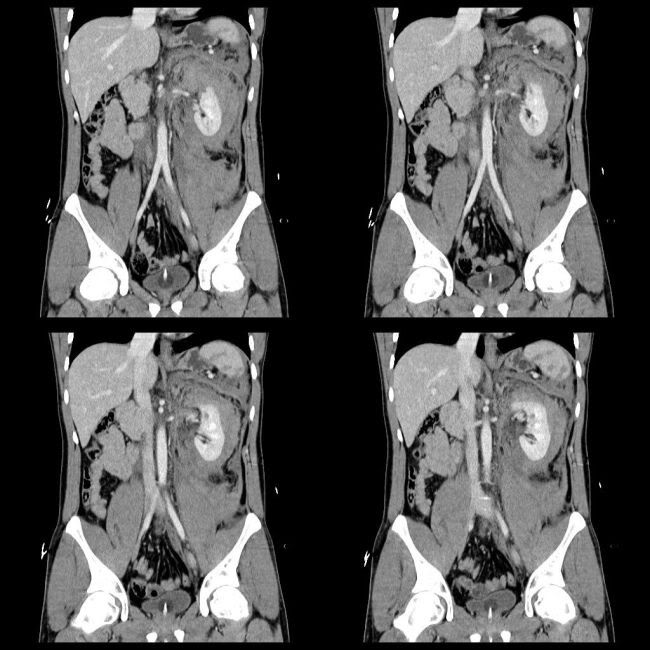
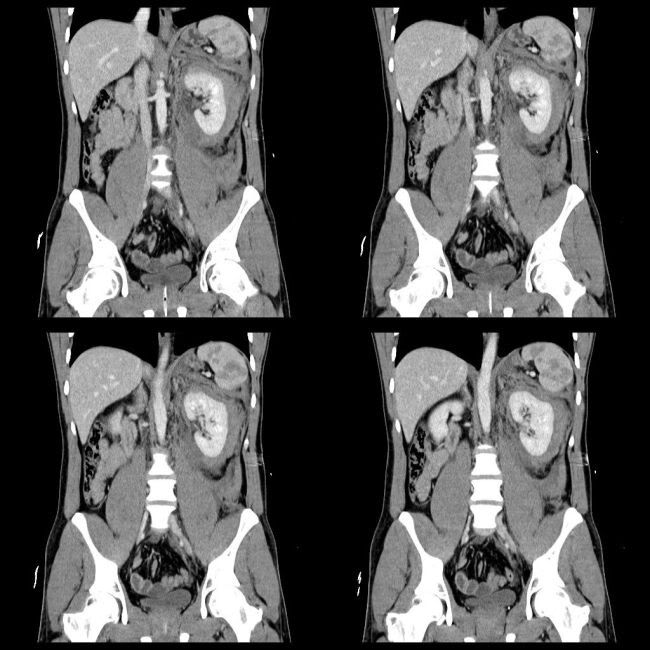
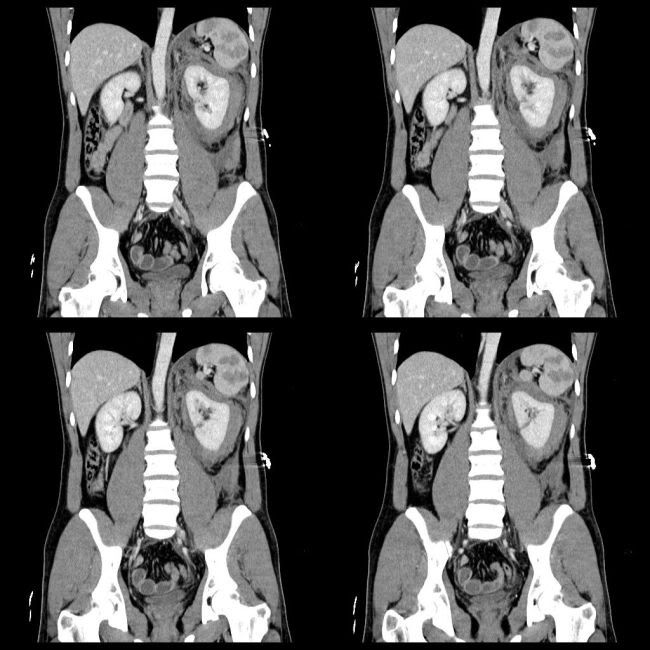
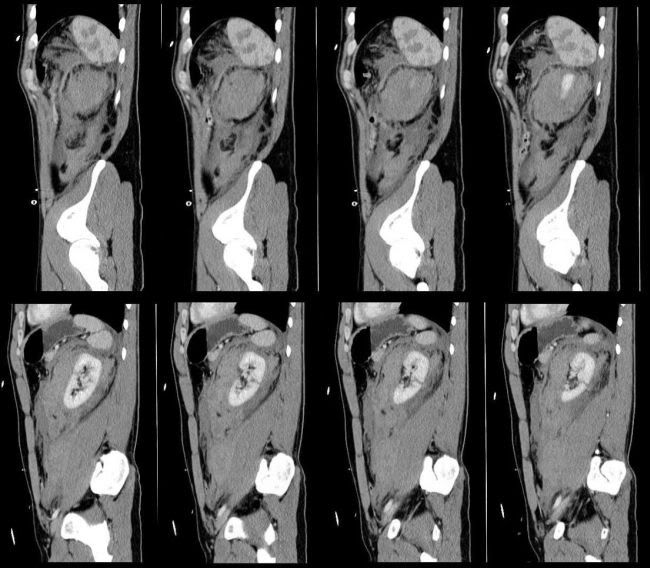
Imaging findings:
1. Left kidney: 2 deep laceration with a large perinephric haemorrhage with haemorrhagic extension into posterior pararenal space. Possible renal vein injury
2. Multiple splenic laceration with small capsular breeches with perisplenic haemorrhage
Discussion:
Splenic injury:
Spleen is most commonly injured solid abdominal organ. Most often due to blunt trauma and often (30-60%) associated with other organ injuries. 25% of left renal injury and 20% of left rib fractures are associated with splenic injury. 40% of splenic lacerations are associated with rib fractures. 20% of splenic injuries occur during surgical procedures. Spontaneous rupture can occur in an abnormal spleen, like in infectious mononucleosus or malaria. Subcapsular hematoma is seen as cresentic/lentiform low attenuation. Parenchymal lacerations are seen as irregularly low attenuation areas. Fracture is seen as complete seperation. Disruption of the capsule causes intraperitoneal hemorrhage. Late complications include splenic pseudocyst.
Grading:
Grade 1 – Minor subcapsular tear or haematoma
Grade 2 – Parenchymal injury not extending to the hilum
Grade 3 – Major parenchymal injury involving vessels and hilum
Grade 4 – Shattered spleen
Management:
Isolated grade 1 and 2 are suitable for conservative management. The patients with cardiovascular instability need surgery, which include repair, spleen conservation surgery (at least 20% of spleen is preserved) and splenectomy. Approximately 30% fail conservative management.
Renal trauma:
Kidney is injured in approximately 8%–10% of blunt or penetrating abdominal injuries. Most of the renal trauma is from blunt injuries (80-90%). Serious renal injuries are frequently associated with injuries to other organs. Multiorgan involvement occurs in 80% of patients with serious penetrating trauma and in 75% of those with blunt trauma. A kidney with preexisting abnormality is at increased risk for injury. About 95% of isolated renal injuries are minor and are managed conservatively. Hematuria is seen in 95% of renal injuries, but absence of hematuria does not exclude renal trauma. Hematuria may be absent in severe renal trauma (25% of renal artery thrombosis may not have hematuria). Hematuria with hypotension is associated with increased risk of significant renal injury; but there is poor correlation between severity of hematuria and severity of renal injury. CT has replaced IVU in the investigation of renal trauma. Indications for CT include gross hematuria, microscopic hematuria with shock, microscopic hematuria with positive peritoneal lavage and microscopic hemauria with significant risk of injury to other organs. CT scanning involves 60-80s delayed and 2-5min delayed dual imaging.
Grading (American Association of Surgeons in Trauma)
1: parenchymal contusions, isolated subcapsular hematoma. 82% of renal injuries.
2: superficial cortical lacerations less than 1 cm deep, nonexpanding perirenal hematoma. 6%
3: lacerations greater than 1 cm deep without extension into collecting system or urinary extravasation. (3 & 4 - 7%)
4: Deep lacerations involving collecting system, traumatic thrombosis of segmental renal arterial branch, injury to main renal artery without devascularization
5: shattered kidney, devascularization - renal artery avulsion, main renal artery thrombosis (shearing injury to intima) (4 & 5 - 5%)
Radiological grading:
1: Minor injury: contusion, intrarenal or subcapsular hematoma, minor lacration with limited perirenal hematoma without extension into collecting system or medulla, subsegmental cortical infarct
2: Major: laceration extending from cortex to medulla/collecting system with/without extravasation, segmental infarct
3: Catastrophic: Multiple lacerations, pedicular injury
4: PUJ avulsion
Imaging findings:
On CT, contusions appear as a focal area of low attenuation with or without defined margins. Acute hematomas are of high attenuation. Small subcapsular hematomas are usually cresentic if small or lentiform if large. Laceration appears as a linear low attenuation. Superficials are less than 1cm and deep are more than 1cm deep. When renal capsule is lacerated, perinephric hemorrhage is usually occurs. Active hemorrhage or pseudoaneurysms are seen as intesne enhancing focal areas; active bleed tracks in the centre of surrounding hemorrhage; false aneurysm is round and focal. Active bleeding is a sign of decompensation (38% in one series) and are candidates for embolization. Urine leak is seen in delayed phase (pyelographic phase - 10 minutes later). Infarcts are wedge shaped low attanutaion traingular structures extending from medulla to cortex and do not enhance. Complete devascularization shows absent nephrogram or cortical rim nephrogram. Thrombosis or laceration of the renal vein is a rare and is type of renal pedicle injury.Venography is preffered as CT may not reliably detect venous laceration. Immediate surgical repair of venous injuries may be required to control bleeding. CT may reveal reveal intraluminal thrombus, nephromegaly, a diminished nephrogram, delayed nephrographic progression, and decreased excretion of contrast material into the collecting system, suggestive of acute venous hypertension.
Management:
Grade 1 to 4 are managed conservatively. The only absolute surgical indication is life-threatening renal bleeding. Relative indications are presence of extensively devitalized tissue (>50% of parenchyma), uncontrolled urinary extravasation even by ureteral stent or nephrostomy, arterial thrombosis. Urine leak spontaneously resolve in up to 90%. Actively bleeding renovascular pedicle injuries (grade 5) need surgical exploration. Traumatic thrombosis or avulsion of renal artery needs repair within 4 hours with success of 14%–29%. If more than 4 hours with normal contralateral kidney they allow it to atrophy.
Early complications occur within 4 weeks and include urinary extravasation and urinoma formation, delayed bleeding, infection of the urinoma, perinephric abscess, sepsis, arteriovenous fistula, pseudoaneurysm and hypertension. Late complications include hydronephrosis, hypertension, calculus formation and chronic pyelonephritis.
References:
1. Fanney DR et al.CT in the diagnosis of renal trauma. RadioGraphics 1990; 10: 29.S201-214
2. Kawashima A et al.Imaging of Renal Trauma: A Comprehensive Review. RadioGraphics 2001; 21: 57
3. Roberts JL et al. CT in abdominal and pelvic trauma. RadioGraphics 1993; 13: 735
No comments:
Post a Comment