Grading:
Grade 1 – Minor subcapsular tear or haematoma
Grade 2 – Parenchymal injury not extending to the hilum
Grade 3 – Major parenchymal injury involving vessels and hilum
Grade 4 – Shattered spleen
Management:
Isolated grade 1 and 2 are suitable for conservative management. The patients with cardiovascular instability need surgery, which include repair, spleen conservation surgery (at least 20% of spleen is preserved) and splenectomy. Approximately 30% fail conservative management.
References:
Roberts JL et al. CT in abdominal and pelvic trauma. RadioGraphics 1993; 13: 735
IMAGE GALLARY:
Patient 1:
Splenic contusion, capsular breech with minimal perisplenic lacerations:
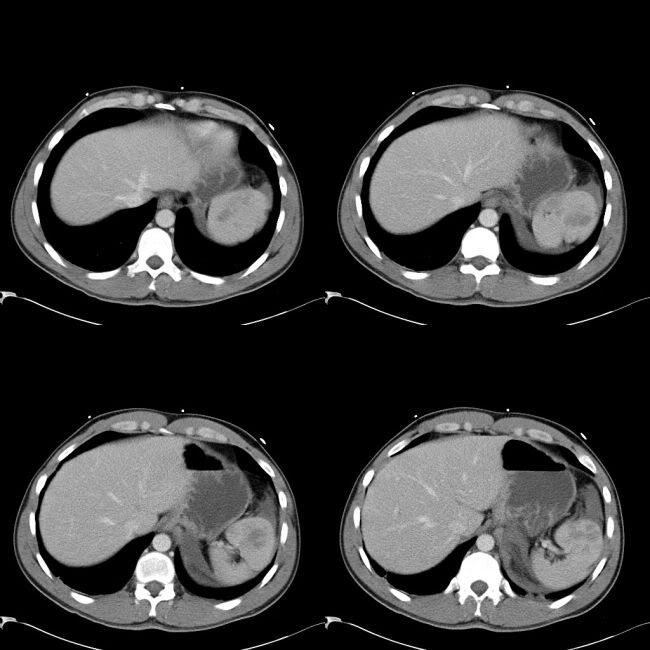
Patient underwent splenectomy.
Patient 2:
Large splenic contusion, capsular breech and large perisplenic collection.
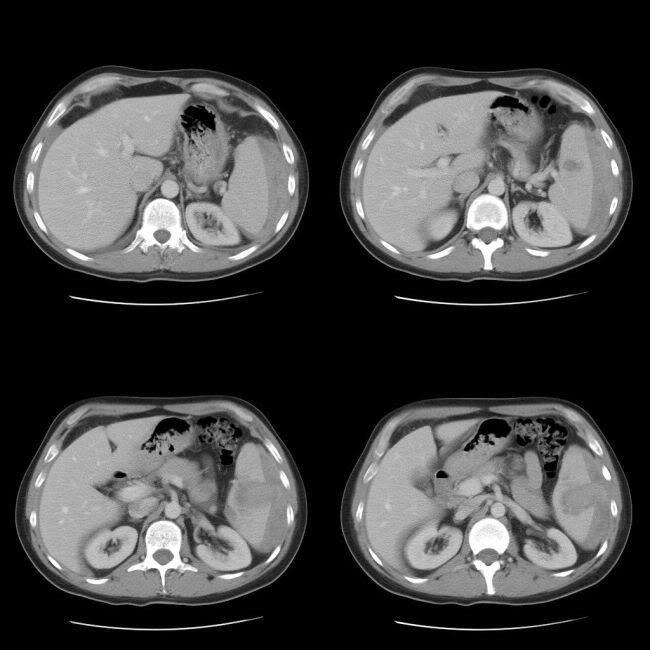
Managed conservatively.
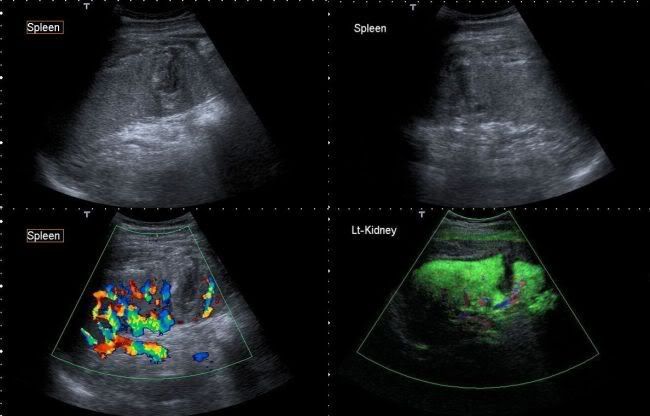
Follow-up ultrasound with microbubble shows a small area of infarct
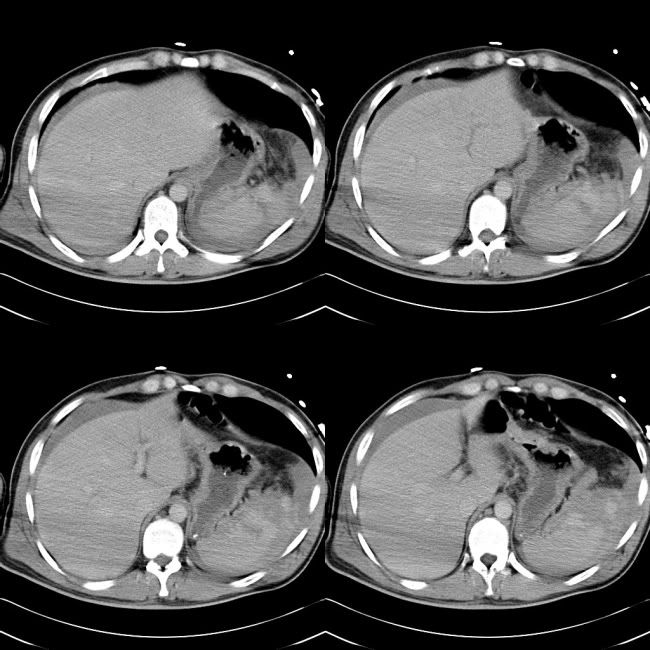
Patient 3: Massive splenic injury
No comments:
Post a Comment