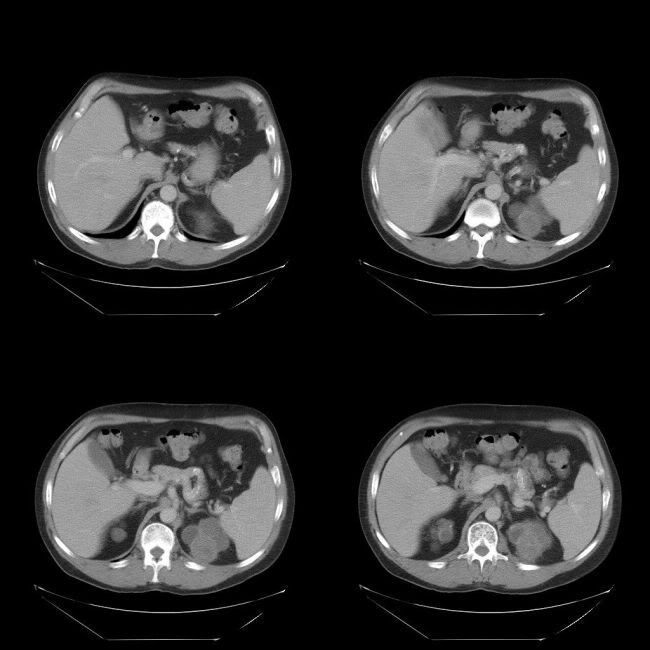
65 year old gentleman with known ADPKD presented with increasing right lumbar pain
Image gallary:



Findings:
ADPKD with hemorrhaic cyst in the right kidney
Did you notice the IVC filter with thrombus at the tip of the IVC filter also?
Discussion:
Flank pain and hematuria may result from cyst hemorrhage or infection, calculi
and renal tumor. There is high association between cyst hemorrhage and flank pain. Differentiation among these complications is important for management purposes. CT is very useful tool in differentiating them.
High density cyst in ADPKD is relatively common finding seen in up to 68% of patients. The larger the size of ADPKD, more the chances of cyst hemorrhage. The factors leading to cyst hemomrhage are possible minor trauma, tight seat belts and spontaneous, possibly related to unsupported sclerotic vessels in the cyst walls. Subcapsular cysts are more likely to bleed.
CT demostrates usually demostrates sharply demarcated homogeneously hyperdense round lesion with smooth margin and no contrast enhancement
They are usually treated by analgeniscs and rest. Sometimes cyst hemorrhage may also cause severe hematunia whihc may need blood transfusion, renal artery embolization and/or nephrectomy.
Reference:
Levine E et al. High-density renal cysts in autosomal dominant polycystic kidney disease demonstrated by CT. Radiology 1985; 154: 477
ANOTHER SIMILAR CASE:
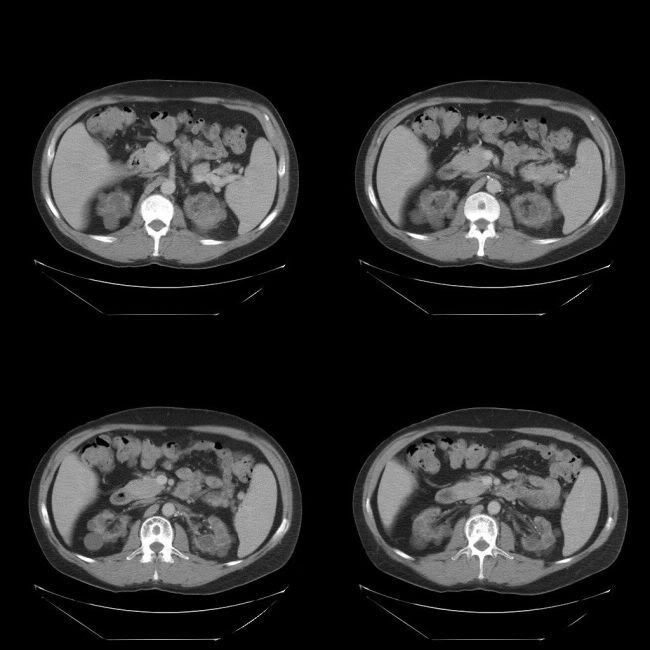
65 year old gentleman with known chronic renal impariment on long term dialysis presented with left flank pain and frank hematuria
Images:
Findings and discussion:
Left upper pole cyst shows increased attenuation, in keeping with cyst hemorrhage. Both kindeys are shrunken and irregular with muleiple cysts, in keeping with chronic renal impairment with long term dialysis. Note the difference in the apeearance of the kindeys in the above case and the present case, although both cases show multiple cysts in both kidneys. The first case is typical for ADPKD and the present one for long term dialysis.
No comments:
Post a Comment